Fill Out a Valid First Report Of Injury Florida Template
When an employee in Florida experiences an injury or illness due to their job, the First Report of Injury or Illness form becomes a critical document, initiating the process for workers' compensation claims. Managed by the Florida Department of Financial Services Division of Workers' Compensation, this form requires detailed information about the employee, including their full name, social security number, date of birth, occupation, and a thorough account of the accident and injury. It also demands precise particulars from the employer, such as the company name, federal ID number, nature of business, and policy number, alongside specifics about the injury event, such as the time, place, and how the injury occurred. Designed to kickstart the claim process, this form serves as a formal notification to the Division, helping ensure injured workers receive the necessary medical attention and financial assistance while they recover. Furthermore, it includes critical data like the physician or hospital name treating the employee, while a stern warning about insurance fraud underscores the form's legality and the seriousness of submitting accurate and truthful information. This framework not only facilitates a structured process for claims but emphasizes the importance of integrity in reporting workplace incidents.
Document Preview Example
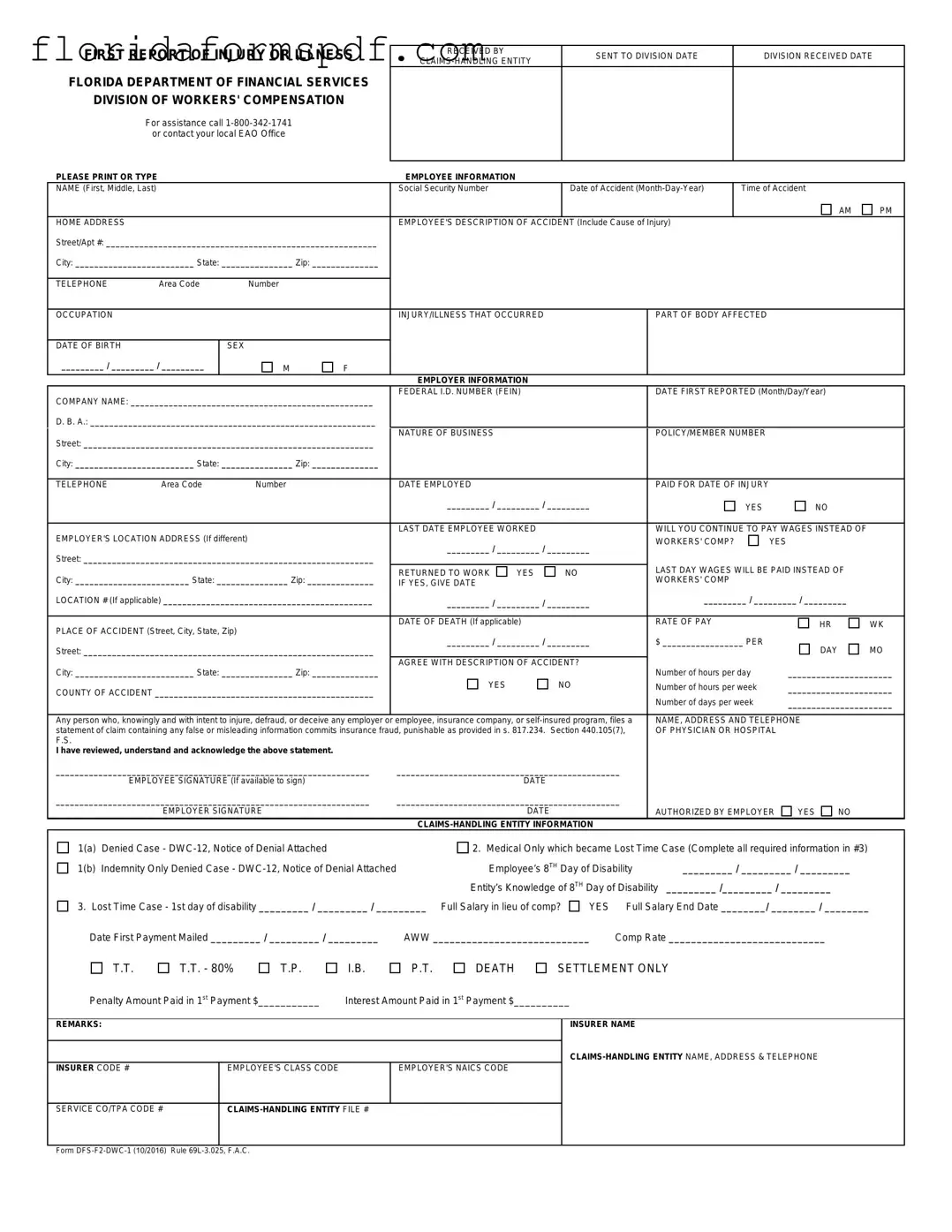
FIRST REPORT OF INJURY OR ILLNESS
FLORIDA DEPARTMENT OF FINANCIAL SERVICES
DIVISION OF WORKERS' COMPENSATION
For assistance call
PLEASE PRINT OR TYPE
RECEIVED BY |
SENT TO DIVISION DATE |
DIVISION RECEIVED DATE |
|
|
|
||
|
|
|
EMPLOYEE INFORMATION
NAME (First, Middle, Last) |
|
|
|
Social Security Number |
|
|
Date of Accident |
|
Time of Accident |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
HOME ADDRESS |
|
|
|
EMPLOYEE'S DESCRIPTION OF ACCIDENT (Include Cause of Injury) |
|
|
|
|
|||||
Street/Apt #: _________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
Area Code |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
OCCUPATION |
|
|
|
INJURY/ILLNESS THAT OCCURRED |
|
|
PART OF BODY AFFECTED |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER INFORMATION |
|
|
|
|
|
|
|
|
|
COMPANY NAME: ___________________________________________________ |
FEDERAL I.D. NUMBER (FEIN) |
|
|
DATE FIRST REPORTED (Month/Day/Year) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||
D. B. A.: ____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
Street: _____________________________________________________________ |
NATURE OF BUSINESS |
|
|
|
POLICY/MEMBER NUMBER |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
TELEPHONE |
Area Code |
Number |
|
DATE EMPLOYED |
|
|
|
PAID FOR DATE OF INJURY |
|
|
|
||
|
|
|
|
_________ / _________ / _________ |
|
|
YES |
|
NO |
|
|||
|
|
|
|
|
|
|
|
|
|
||||
EMPLOYER'S LOCATION ADDRESS (If different) |
|
LAST DATE EMPLOYEE WORKED |
|
|
WILL YOU CONTINUE TO PAY WAGES INSTEAD OF |
|
|||||||
|
_________ / _________ / _________ |
WORKERS' COMP? |
|
YES |
|
||||||||
|
|
|
|
|
|
||||||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|||||||
|
|
|
|
LAST DAY WAGES WILL BE PAID INSTEAD OF |
|
||||||||
|
|
|
|
RETURNED TO WORK |
YES |
|
NO |
|
|||||
City: ________________________ State: _______________ Zip: ______________ |
|
WORKERS' COMP |
|
|
|
|
|||||||
IF YES, GIVE DATE |
|
|
|
|
|
|
|
||||||
LOCATION # (If applicable) ____________________________________________ |
_________ / _________ / _________ |
_________ / _________ / _________ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
RATE OF PAY |
|
|
|
|
||
PLACE OF ACCIDENT (Street, City, State, Zip) |
|
DATE OF DEATH (If applicable) |
|
|
|
|
HR |
WK |
|||||
|
|
|
|
|
|
|
|
|
|||||
|
_________ / _________ / _________ |
$ _________________ PER |
|
|
|
||||||||
Street: _____________________________________________________________ |
|
DAY |
MO |
||||||||||
|
|
|
|
|
|
|
|
||||||
City: _________________________ State: _______________ Zip: ______________ |
AGREE WITH DESCRIPTION OF ACCIDENT? |
Number of hours per day |
______________________ |
||||||||||
|
|
|
|
||||||||||
COUNTY OF ACCIDENT ______________________________________________ |
YES |
|
NO |
Number of hours per week |
______________________ |
||||||||
|
|
|
|
Number of days per week |
______________________ |
||||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|||||||||
Any person who, knowingly and with intent to injure, defraud, or deceive any employer or |
employee, insurance company, or |
NAME, ADDRESS AND TELEPHONE |
|
||||||||||
statement of claim containing any false or misleading information commits insurance fraud, punishable as provided in s. 817.234. Section 440.105(7), |
OF PHYSICIAN OR HOSPITAL |
|
|||||||||||
F.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
I have reviewed, understand and acknowledge the above statement.
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYEE SIGNATURE (If available to sign) |
DATE |
|
|
|
|
|
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYER SIGNATURE |
DATE |
|
AUTHORIZED BY EMPLOYER |
YES |
NO |
|
|
|
|
|
|
|
||
1(a) |
Denied Case - |
2. Medical Only which became Lost Time Case (Complete all required information in #3) |
|||||
1(b) |
Indemnity Only Denied Case - |
Employee’s 8TH Day of Disability |
_________ / _________ / _________ |
||||
|
|
Entity’s Knowledge of 8TH Day of Disability |
_________ /_________ / _________ |
|
|||
3. Lost Time Case - 1st day of disability _________ / _________ / _________ Full Salary in lieu of comp? |
YES |
Full Salary End Date ________/ ________ / ________ |
|||||
Date First Payment Mailed _________ / _________ / _________ |
AWW ____________________________ |
Comp Rate ____________________________ |
|
||||
T.T.
T.T. - 80%
T.P.
I.B.
P.T.
DEATH
SETTLEMENT ONLY
Penalty Amount Paid in 1st Payment $___________ |
Interest Amount Paid in 1st Payment $__________ |
REMARKS:
INSURER CODE # |
EMPLOYEE'S CLASS CODE |
EMPLOYER'S NAICS CODE |
|
|
|
INSURER NAME
SERVICE CO/TPA CODE #
Form
The collection of the social security number on this form is specifically authorized by Section 440.185(2), Florida Statutes. The social security number will be used as a unique identifier in Division of Workers' Compensation database systems for individuals who have claimed benefits under Chapter 440, Florida Statutes. It will also be used to identify information and documents in those database systems regarding individuals who have claimed benefits under Chapter 440, Florida Statutes, for internal agency tracking purposes and for purposes of responding to both public records requests and subpoenas that require production of specified documents. The social security number may also be used for any other purpose specifically required or authorized by state or federal law.
Document Overview
| Fact Name | Detail |
|---|---|
| Governing Law | Chapter 440, Florida Statutes |
| Managing Department | Florida Department of Financial Services Division of Workers' Compensation |
| Assistance Contact Information | 1-800-342-1741 or local EAO Office |
| Form Identification | DFS-F2-DWC-1 (10/2016), Rule 69L-3.025, F.A.C. |
Instructions on How to Fill Out First Report Of Injury Florida
Filling out the First Report of Injury or Illness form is a crucial step in notifying the Florida Department of Financial Services - Division of Workers' Compensation about a workplace injury or illness. This process ensures the proper documentation is filed, which is essential for the injured employee to receive any possible workers' compensation benefits. The following step-by-step instructions have been prepared to guide you through completing this form accurately.
- Write the date the form is being filled out in the "DATE" section under "RECEIVED BY."
- Enter the date the form is sent to the Division in the "SENT TO DIVISION DATE" field.
- Under "CLAIMS-HANDLING ENTITY," provide the name of the entity managing the workers' compensation claims.
- In the "EMPLOYEE INFORMATION" section, fill in the employee's full name, Social Security Number, date of the accident, time of accident (checking AM or PM as appropriate), and the employee's home address including street/apartment number, city, state, and zip code.
- Under "TELEPHONE," add the employee's contact number with the area code.
- For the "OCCUPATION" slot, specify the employee's job role at the time of the injury or illness.
- Indicate the nature of the injury or illness and the part of the body affected.
- Fill in the employee's date of birth and check the appropriate box for sex.
- In "EMPLOYER INFORMATION," provide the company name, federal I.D. number (FEIN), the date the injury was first reported, and any doing-business-as (D.B.A.) name if applicable.
- Enter the employer's address, nature of business, and policy/member number, including the city, state, zip code, and contact number.
- Detail the employee's employment information such as the date employed, if they were paid for the date of the injury, and if the employer will continue to pay wages in lieu of workers' compensation. Include the last date the employee worked.
- If the employee has returned to work, indicate this by checking "YES" or "NO" and provide the date of return if applicable.
- Specify the rate of pay at the time of injury or illness.
- Provide the place of the accident (street, city, state, zip) and if known, the date of death related to the injury or illness.
- Assess whether you agree with the employee's description of the accident and check "YES" or "NO."
- Under "NAME, ADDRESS AND TELEPHONE OF PHYSICIAN OR HOSPITAL," provide details about the initial medical provider or hospital that treated the employee.
- If available, have the employee sign and date the form.
- The employer or authorized representative should then sign and date the form, indicating if the signature was authorized by the employer.
- Complete the "CLAIMS-HANDLING ENTITY INFORMATION" as it applies to the case specifics, including dates of disability, knowledge of the 8th day of disability, and any compensation information available.
- Lastly, fill in the "REMARKS" section with any additional observations or noteworthy information not covered elsewhere on the form.
After you've filled out the form, it must be submitted to the Division of Workers' Compensation as part of the claims process. This step is vital in initiating the workers' compensation procedure, which can provide financial assistance and support to the injured employee during their recovery period.
Listed Questions and Answers
What is the purpose of the First Report of Injury or Illness form in Florida?
The First Report of Injury or Illness form serves as a vital document in the Florida workers' compensation system. It is used to report any work-related injury or illness to the Florida Department of Financial Services' Division of Workers' Compensation. This form initiates the process for an injured employee to potentially receive benefits. It collects all necessary information about the employee, the employer, and details of the accident or illness, ensuring timely and efficient processing of workers' compensation claims.
How soon must the First Report of Injury or Illness form be filed?
It is imperative that the First Report of Injury or Illness form is filed as soon as possible after the occurrence of a work-related injury or illness. The State of Florida mandates that employers report these incidents to their workers' compensation insurance carrier within seven days of learning about the injury or illness. Following this, the insurance carrier has an additional seven days to forward the report to the Florida Division of Workers' Compensation. Prompt filing is crucial to the swift handling of the claim.
Who is responsible for filing this form?
The employer bears the primary responsibility for filing the First Report of Injury or Illness form. When an employee reports an injury or illness that occurred in the workplace or while performing work-related duties, the employer must then report this information to their workers' compensation insurance provider using this form. The insurance provider will then complete the claims process by submitting the form to the Florida Division of Workers' Compensation.
Can an employee file the First Report of Injury form if the employer fails to do so?
Yes, if an employer neglects to file the First Report of Injury or Illness form, the injured or ill employee has the right to file the form independently. Employees can contact the Florida Division of Workers' Compensation directly for assistance in submitting the form. This ensures that the employee's right to pursue workers' compensation benefits is preserved, irrespective of the employer's action or inaction.
What details are required on the First Report of Injury or Illness form?
The form requires comprehensive information that includes the employee's name, social security number, date of birth, and contact information, along with the employer's details, such as the company name, address, and federal identification number (FEIN). It also demands specifics about the injury or illness, including the date, time, and location of the incident, a description of how the injury or illness occurred, and the nature and extent of the injuries or illness. Additionally, information on the treating physician or hospital must be provided where applicable.
What happens after the First Report of Injury or Illness form is filed?
Once the First Report of Injury or Illness form is filed, it is reviewed by the employer's workers' compensation insurance carrier and the Florida Division of Workers' Compensation. This initiates the process for determining the eligibility of the employee for workers' compensation benefits. The injured or ill employee may be contacted for additional information or clarification. If approved, benefits for medical treatment, wage replacement, or other forms of compensation may be provided according to Florida's workers' compensation laws.
Common mistakes
Filling out the First Report of Injury or Illness Florida form correctly is crucial to ensure the process runs smoothly and the employee gets the benefits they're entitled to. However, people often make mistakes, which can delay or complicate the claims process. Here are nine common mistakes:
- Not double-checking the employee’s personal information: Ensuring the employee's name, social security number, and home address are correct is fundamental. Mistakes here can lead to significant delays.
- Incorrectly reporting the date and time of the accident: The date and time of the accident are critical for a claim. Using the wrong date or time can cause confusion and delay the processing of the claim.
- Failing to provide a detailed description of the accident: A thorough account of how the accident happened is crucial. Vague descriptions can lead to misunderstandings about the nature of the injury or illness.
- Omitting parts of the body affected: Clearly listing all the parts of the body that were injured or affected is necessary for a proper assessment and treatment plan.
- Leaving the employer’s information incomplete: Accurately filling out the employer's information, including the company name and contact information, ensures the claim is processed efficiently.
- Forgetting to report the nature of the business: The nature of the employer's business can be relevant, especially if the injury or illness is specific to certain types of work.
- Not specifying if wages will be continued instead of workers' comp: It's important to state whether the employer will continue to pay wages after the injury. This affects how compensation is calculated.
- Ignoring the physician or hospital information: Right after an injury, it might seem challenging to provide this, but updating the form with the physician or hospital details as soon as possible is vital for processing the claim.
- Forgetting to sign the document: An unsigned form can lead to unnecessary delays. Ensure both the employee and employer sign the form to validate the information provided.
Accurate and complete documentation on the First Report of Injury or Illness form helps expedite the claims process and ensures that employees receive the benefits and care they need without undue delay.
Documents used along the form
When dealing with the First Report of Injury or Illness in Florida, a comprehensive approach often involves several other crucial documents. These forms and documents play a vital role in ensuring the smooth processing of workers' compensation claims, providing detailed information necessary for accurate assessments and timely support for the injured or ill worker. Let’s delve into some of these crucial documents often accompanying the First Report of Injury form.
- DWC-12, Notice of Denial: This form is essential in cases where a workers' compensation claim is denied by the claims-handling entity. It outlines the reasons for denial, providing the employee with clear information on why their claim was not accepted and what further actions they may consider.
- Wage Statement (Form DWC-3): This document is critical for determining the compensation rate for an injured or ill worker. It details the employee's wages prior to the injury or illness, enabling accurate calculation of benefits based on their earnings.
- Employee’s Claim for Workers’ Compensation Benefits (DWC-1 Form): Although it seems similar to the First Report of Injury form, this document is filled out by the employee to formally claim workers' compensation benefits. It includes detailed information about the injury or illness from the employee’s perspective.
- Pre-Authorization Request for Treatment Form: Before certain types of medical treatments can be provided under workers' compensation, they must be pre-authorized. This form is used by healthcare providers to request approval for specific treatments, ensuring they are covered under the worker’s compensation claim.
- Medical Reports: Detailed reports from physicians or hospitals treating the injured or ill worker are crucial. These documents provide insights into the nature of the injury or illness, the treatment provided, and the expected outcomes. They are vital for assessing the claim and determining the benefits due.
Understanding and managing these documents is paramount in navigating the complexities of workers’ compensation claims in Florida. They ensure that all parties are well-informed and contribute to a transparent, efficient process. Accurate completion and timely submission of these forms facilitate a smoother claim process, ultimately aiding in the recovery and support of the injured or ill worker.
Similar forms
The First Report of Injury Florida form is similar to other documents used in workers' compensation and employer insurance reporting. These documents share a focus on capturing detailed information about an injury or illness that occurs at the workplace, aiming to streamline the process for claims and support for the affected employee. Among these similar documents are the OSHA Form 300 and the Employer's Report of Industrial Injury.
The OSHA Form 300, or the 'Log of Work-Related Injuries and Illnesses', closely mirrors the Florida form in its aim to document every significant work-related injury or illness. Both forms require detailed information about the employee, the nature of the job, and specifics of the injury or illness, including how it occurred. However, the OSHA Form 300 is part of a broader requirement for employers to keep a running log over the year, whereas the First Report of Injury form is filed per incident. Both play a crucial role in maintaining workplace safety and health compliance, aiding in identifying risky areas or practices within the workplace.
The Employer's Report of Industrial Injury is another document similar to the Florida form, typically used in various states to report workplace injuries or illnesses to the appropriate workers' compensation board or authority. Like the First Report of Injury Florida form, it collects comprehensive information about the injured or ill employee, the circumstances of the accident, and the immediate response. Differences may arise in the specific details requested by each state's form, reflecting unique regulatory requirements or procedures for processing workers' compensation claims. Yet, the fundamental goal remains consistent: to ensure that incidents are accurately reported and that employees receive the appropriate care and benefits promptly.
Dos and Don'ts
Things You Should Do:
- Be Thorough: Provide detailed and precise information about the injury or illness. This includes the exact location and description of the accident, ensuring all details are clear and specific.
- Check for Accuracy: Double-check all the information for any mistakes. This includes verifying the correct dates, times, and spelling of all names and locations.
- Report in a Timely Manner: File the report as soon as possible after the accident occurs. Timely reporting can impact the processing and outcome of the claim.
- Include Complete Employee Information: Make sure to fill out all employee information sections, including the social security number, as it’s a unique identifier used in the Division of Workers' Compensation database systems.
- Describe the Accident Accurately: Give a clear and precise employee’s description of the accident and the cause of injury, including what happened and how it happened.
- Sign the Form: Ensure that both the employee (if available to sign) and the employer sign the form. This attests to the accuracy and acknowledgment of the information provided.
Things You Shouldn’t Do:
- Avoid Guesswork: Do not guess or make assumptions about any piece of information. If you are unsure about a detail, it's better to check your facts before submitting the form.
- Don’t Leave Blanks: Avoid leaving any section of the form blank. If a section does not apply, make sure to mark it as “N/A” instead of leaving it empty.
- Avoid Delay in Reporting: Do not delay filling out and submitting the form. Delaying can lead to fines and penalties, apart from potentially affecting the claim's processing.
- Skip Using Abbreviations: Avoid using abbreviations or industry jargon that might not be understood by the claims processor. Use clear and simple language.
- Don’t Provide Incomplete Descriptions: Avoid giving vague descriptions of the incident. Lack of detail can lead to unnecessary delays and possible disputes during the claim process.
- Refrain from Altering the Form: Do not alter the form structure or questions in any way. Altering the form could lead to miscommunication or even rejection of the form.
By adhering to these guidelines, you can fill out the First Report of Injury or Illness form accurately and efficiently, aiding the smooth proceeding of the claims process.
Misconceptions
Many people have misconceptions about the First Report of Injury or Illness (DWC-1) form in Florida, which can lead to confusion and delay in the claims process. Here are nine common myths debunked:
- Only severe injuries need to be reported: All workplace injuries or illnesses, regardless of their severity, should be reported using the DWC-1 form to ensure proper documentation and potential coverage of workers’ compensation benefits.
- Employees can't file if they don't have all the information: While it's important to provide as much detail as possible, an employee should not delay filing the DWC-1 form due to missing information. Updates can be made as more details become available.
- The reporting deadline is flexible: Florida law requires that the injury or illness be reported as soon as possible but no later than 30 days from the date of the accident, discovery of the injury/illness, or from the date, the employee knew or should have known the injury/illness was work-related. Missing this deadline can jeopardize benefit eligibility.
- Filing a DWC-1 form guarantees compensation: Submission of the DWC-1 form initiates the process but does not guarantee that the claim will be accepted or that benefits will be provided. Claims undergo evaluation for adherence to eligibility criteria.
- Only the employer can complete the form: Although employers play a crucial role in reporting workplace injuries, both the employee and employer have sections to complete on the DWC-1 form to ensure the claim is processed correctly.
- The form must be submitted in person: While in-person submission might be an option, the DWC-1 form can also be sent to the Division of Workers' Compensation electronically or by mail, offering flexibility and convenience for both employees and employers.
- Private information is at risk: The collection and handling of sensitive information such as social security numbers are protected by privacy laws. This information is used responsibly by the Division of Workers' Compensation to accurately process and track claims.
- Reporting an injury will automatically lead to increased insurance premiums: This is not always the case. Premiums are influenced by a variety of factors, and a single claim does not necessarily dictate a premium increase. Risk management practices and claims history play significant roles in premium calculation.
- The DWC-1 form is the only step in the claim process: Completing and submitting the DWC-1 form is just the beginning. Employees may need to provide additional documentation, undergo medical examinations, and participate in other claim-related activities as the process moves forward.
Understanding the purpose and process of the DWC-1 form is crucial for both employees and employers in Florida. Dispelling these misconceptions can help ensure timely and accurate reporting of workplace injuries or illnesses, facilitating a smoother workers' compensation claims process.
Key takeaways
- Filling out the First Report of Injury or Illness form is a crucial step for initiating a workers' compensation claim in Florida, ensuring that injured workers may receive benefits and support promptly.
- It is required by the Florida Department of Financial Services' Division of Workers' Compensation, highlighting the importance of timely and accurate reporting by employers.
- The form requests detailed employee information, including name, social security number, date and time of the accident, and a description of the accident and injury, emphasizing the need for precise and comprehensive documentation.
- Employer information, such as company name, federal ID number, and policy number, is also required, underscoring the employer's role in the claims process.
- The section regarding the injury or illness and part of the body affected necessitates clear and specific details to avoid any ambiguity that could delay claim processing.
- An employee's signature is requested when available, underscoring the importance of the injured worker's acknowledgment and agreement with the information submitted.
- The form includes a provision for reporting wage continuation options by the employer, which plays a crucial role in determining how benefits are calculated and delivered.
- Accuracy is paramount when filling out this form as it contains a warning about insurance fraud, emphasizing the serious legal implications of submitting false or misleading information.
- The form serves multiple purposes, including as an initial claim report for workers' compensation benefits and as a legal document that can be used in dispute resolution.
- There's a DWC-1 Purpose and Use Statement that clarifies the collection and use of social security numbers, ensuring compliance with Florida statutes and highlighting the protective measures taken to safeguard personal information.
- The document also outlines specific actions and due dates following the acknowledgment of disability or time lost from work, guiding employers through subsequent steps in the claims handling process.
Popular PDF Documents
Department Of Corrections Visitation Florida - Get one step closer to reuniting with loved ones in Florida facilities by submitting the required visitor information on the Department of Corrections form.
How to Get Power of Attorney in Florida - The form acts as a safeguard for the vehicle owner, outlining the exact powers being granted and limiting them to specific vehicle-related actions.
Florida Family Court - To avoid processing delays, all information should be submitted by March 1st for the current tax year exemptions.