Fill Out a Valid Florida Dh 1777 Template
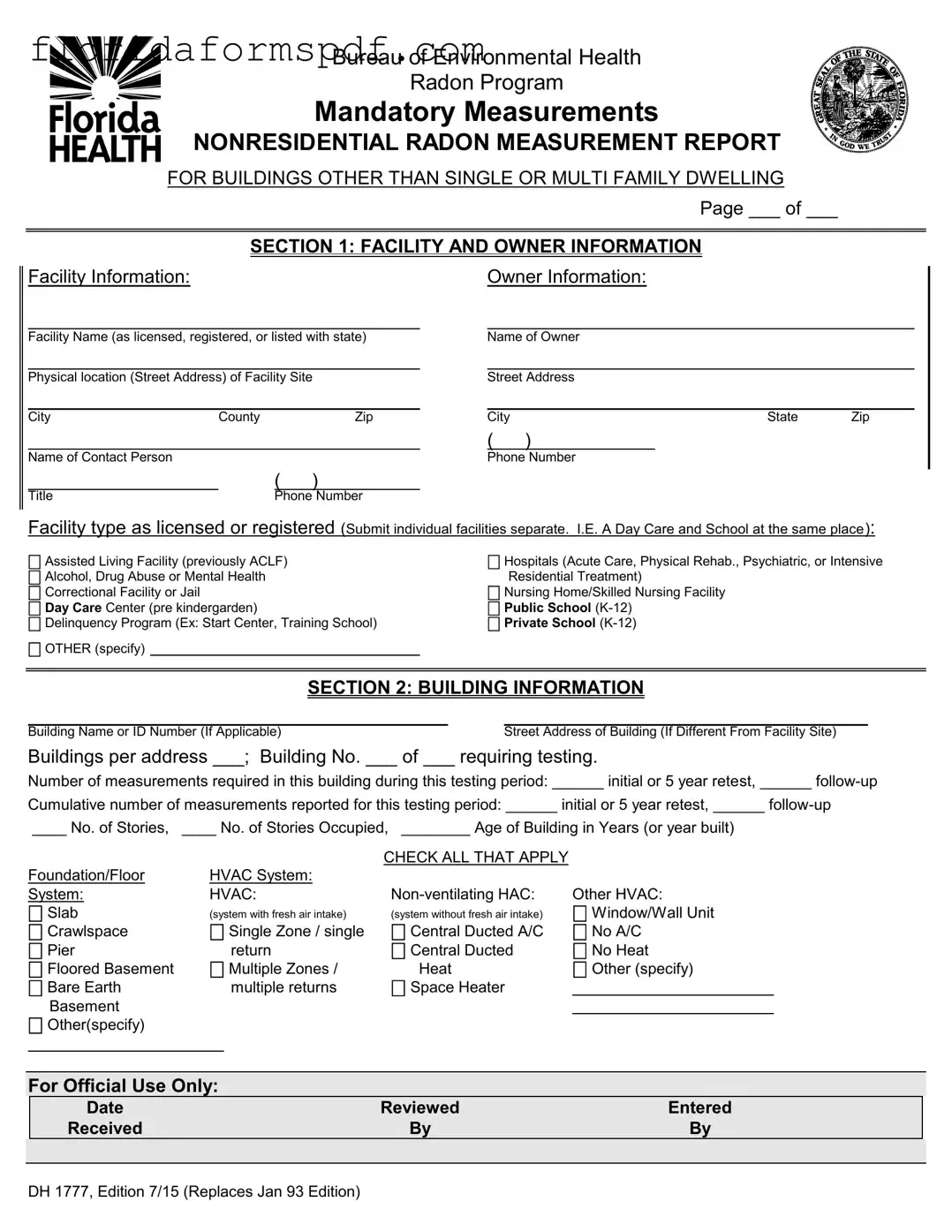
In the realm of ensuring public health and safety within nonresidential spaces in Florida, the meticulous documentation of radon levels is a crucial responsibility upheld by the Florida Department of Health. The Florida DH 1777 form serves as an essential tool in this regard, mandating the systematic reporting of radon measurements in buildings other than single or multi-family dwellings. Designed to capture detailed information ranging from facility and owner specifics to the intricate aspects of building structure and the HVAC systems in place, the form facilitates a comprehensive understanding of the radon measurement activities conducted. It caters to a variety of facilities such as assisted living facilities, hospitals, schools, and correctional facilities, among others, ensuring a broad applicability across different nonresidential environments. Additionally, the form divides the reporting process into several sections, including facility and owner information, building information, measurement results, and details about the measurement process—whether it was carried out by a certified radon measurement business or by staff employed by the facility. The inclusion of certification details for individuals or businesses conducting the tests underscores the form’s emphasis on the credibility and accuracy of the radon measurements reported. This structured approach not only aids in maintaining health standards but also serves as a regulatory compliance measure, aligning with the Florida Administrative Code and Florida Statutes. The procedural finalization of submitting the form, complete with certification by an authorized facility representative, ensures that the data reaches the Department of Health’s Bureau of Environmental Health/Radon Program efficiently, reinforcing the state’s commitment to protecting its citizens from the potential risks associated with radon exposure.
Document Preview Example
Bureau of Environmental Health
Radon Program
Mandatory Measurements
NONRESIDENTIAL RADON MEASUREMENT REPORT
FOR BUILDINGS OTHER THAN SINGLE OR MULTI FAMILY DWELLING
Page ___ of ___
SECTION 1: FACILITY AND OWNER INFORMATION
Facility Information: |
Owner Information: |
Facility Name (as licensed, registered, or listed with state)
Physical location (Street Address) of Facility Site
City |
County |
Zip |
Name of Contact Person
Name of Owner
Street Address
City |
State |
Zip |
()
Phone Number
()
TitlePhone Number
Facility type as licensed or registered (Submit individual facilities separate. I.E. A Day Care and School at the same place):
Assisted Living Facility (previously ACLF) |
Hospitals (Acute Care, Physical Rehab., Psychiatric, or Intensive |
|
Alcohol, Drug Abuse or Mental Health |
Residential Treatment) |
|
Correctional Facility or Jail |
Nursing Home/Skilled Nursing Facility |
|
Day Care Center (pre kindergarden) |
Public School |
|
Delinquency Program (Ex: Start Center, Training School) |
Private School |
|
OTHER (specify) |
|
|
|
|
|
|
|
|
|
|
|
SECTION 2: BUILDING INFORMATION
Building Name or ID Number (If Applicable)Street Address of Building (If Different From Facility Site)
Buildings per address ___; Building No. ___ of ___ requiring testing.
Number of measurements required in this building during this testing period: ______ initial or 5 year retest, ______
Cumulative number of measurements reported for this testing period: ______ initial or 5 year retest, ______
____ No. of Stories, ____ No. of Stories Occupied, ________ Age of Building in Years (or year built)
Foundation/Floor
System:
Slab
Crawlspace
Pier
Floored Basement
Bare Earth Basement
Other(specify)
|
CHECK ALL THAT APPLY |
|
HVAC System: |
|
|
HVAC: |
Other HVAC: |
|
(system with fresh air intake) |
(system without fresh air intake) |
Window/Wall Unit |
Single Zone / single |
Central Ducted A/C |
No A/C |
return |
Central Ducted |
No Heat |
Multiple Zones / |
Heat |
Other (specify) |
multiple returns |
Space Heater |
|
|
||
|
|
|
For Official Use Only:
|
Date |
Reviewed |
Entered |
|
|
Received |
By |
By |
|
|
|
|
|
|
DH 1777, Edition 7/15 (Replaces Jan 93 Edition)
|
|
|
|
|
|
|
SECTION 3: RESULTS |
|
|
|
|
|||||
Measurement Type: Initial or 5 Year Retest, |
|
|
|
|
||||||||||||
Dates of Measurement: FROM |
/ / |
|
TO |
/ / |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Name of Person who performed Measurement (Placed Device) |
|
† |
|
|
Certificate No. (If Applicable) |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
‡ |
||||
|
Story |
|
Room |
Result |
|
Units |
|
Device |
|
|
Time in Hours |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
† P for pCi/L or W for WL
‡
SECTION 4
COMPLETE ONLY IF MEASUREMENTS ARE PERFORMED BY A RADON MEASUREMENT BUSINESS
Name of Business and Cert. No. |
Name of Specialist and Cert. No. |
Signature of Specialist
SECTION 5
COMPLETE ONLY IF MEASUREMENTS ARE PERFORMED BY STAFF EMPLOYED BY THE FACILITY
I hereby certify that the Radon measurements reported herein have been performed in accordance with Chapter
Authorized Representative of Facility |
|
Date |
Upon completion of this form, send to:
Department of Health
Bureau of Environmental Health / Radon Program
4052 Bald Cypress Way, Bin #A12
Tallahassee, FL
You may scan the report and email it to RadonReports@FLhealth.gov
For Assistance in Completing this Form call
Document Overview
| Fact | Detail |
|---|---|
| Form Title | Florida DH 1777 Form |
| Purpose | Mandatory Measurements NONRESIDENTIAL RADON MEASUREMENT REPORT FOR BUILDINGS OTHER THAN SINGLE OR MULTI FAMILY DWELLING |
| Sections Included | Facility and Owner Information, Building Information, Results, Information on Measurement by Radon Measurement Business, Certification by Facility’s Authorized Representative |
| Applicable Facilities | Assisted Living Facility, Hospitals, Correctional Facility or Jail, Day Care Center, Public and Private Schools among others |
| Scope of Application | Used in the state of Florida for nonresidential buildings to report radon levels |
| Governing Laws | Chapter 64E-5, Florida Administrative Code, and Chapter 404, Florida Statutes |
| Submission Information | Completed forms should be sent to the Department of Health Bureau of Environmental Health / Radon Program in Tallahassee, FL or emailed to RadonReports@FLhealth.gov |
| Assistance Contact | 1-800-543-8279 for help in completing the form |
Instructions on How to Fill Out Florida Dh 1777
Filling out the Florida DH 1777 form is a straightforward process if you have all the necessary information at hand. It is designed to report radon measurements in facilities other than single or multi-family dwellings. See the steps below on how to properly fill out this form to ensure compliance and accuracy of the information provided.
- Start with Section 1: Facility and Owner Information. Enter the facility's name as it is licensed, registered, or listed with the state. Fill out the physical location, city, county, and zip code of the facility. Add the name and phone number of the contact person, and repeat this process for the owner's information.
- Proceed to Facility Type: Check the appropriate box that describes the type of facility being reported. If your facility type is not listed, select "OTHER" and specify in the space provided.
- Move to Section 2: Building Information. If applicable, write the building name or ID number. For buildings at a different location from the facility site, provide the street address. Indicate the number of buildings per address and the number of the building requiring testing. Enter the number of measurements required and the cumulative number of measurements reported for this testing period. Fill in the number of stories, the number of stories occupied, and the age of the building or year built. Check the appropriate boxes for the foundation/floor system and HVAC system present in the building.
- Continue to Section 3: Results. Choose the type of measurement (initial, 5-year retest, or follow-up) and fill in the dates of measurement. Provide the name of the person who performed the measurement and their certificate number if applicable, along with the story, room, result, units, device, and time in hours. Ensure to indicate the measurement's units and specify the device type used.
- If applicable, complete Section 4: This section is only required if the measurements are performed by a radon measurement business. Fill in the name of the business and certification number, as well as the name of the specialist, their certification number, and the specialist's signature.
- If measurements are performed by staff employed by the facility, complete Section 5: An authorized representative of the facility must certify that the radon measurements reported comply with Chapter 64E-5, Florida Administrative Code, and Chapter 404, Florida Statutes. This requires the authorized representative’s signature and the date of certification.
- Final Step: Upon completion, send the form to the Department of Health Bureau of Environmental Health / Radon Program at the address listed or email it to the provided email address. If you need assistance completing the form, the given phone number can be called for support.
By following these steps diligently, you'll ensure that the DH 1777 form is filled correctly and thoroughly, paving the way for a smooth submission to the Department of Health.
Listed Questions and Answers
What is the purpose of the Florida DH 1777 form?
The Florida DH 1777 form is used for reporting radon measurement results in nonresidential buildings other than single or multi-family dwellings. This includes facilities such as schools, daycare centers, hospitals, correctional facilities, and other types designated on the form. The objective is to ensure these environments adhere to safety standards for radon levels, safeguarding occupants' health.
How often must radon measurements be reported using the Florida DH 1777 form?
Radon measurements must be reported at the initial assessment and then every five years for retesting, as outlined in the form. Additionally, follow-up measurements may be required if initial results indicate radon levels that exceed the recommended safety thresholds. These procedures align with Chapter 64E-5, Florida Administrative Code, and Chapter 404, Florida Statutes, ensuring continuous monitoring and compliance.
Can I submit the Florida DH 1777 form electronically?
Yes, you can submit the Florida DH 1777 form electronically. Upon completing the form, you have the option to scan the report and email it to RadonReports@FLhealth.gov, as indicated in the document's instructions. This digital submission method offers a convenient alternative to mailing the physical form to the Department of Health, Bureau of Environmental Health / Radon Program in Tallahassee.
Who is authorized to perform radon measurements reported on the Florida DH 1777 form?
Radon measurements reported on the Florida DH 1777 form must be performed by either a certified radon measurement business or by staff employed by the facility, provided they comply with Chapter 64E-5, Florida Administrative Code, and Chapter 404, Florida Statutes. The form requests specific details, including the name and certificate number of the person or business conducting the measurement, to verify qualifications and ensure adherence to regulatory standards.
Common mistakes
Filling out the Florida DH 1777 form, which is a mandatory measurement report for nonresidential radon levels, can be a complex process. It requires careful attention to detail to ensure accuracy and compliance with regulations. However, some common mistakes often occur during the process, which can lead to issues with the submission or the accuracy of the reported data. Here are six mistakes people frequently make when completing this form:
Incorrect facility type selection: Many individuals mistakenly choose the wrong facility type from the provided options. Each facility type, such as Assisted Living Facility or Day Care Center, has specific testing requirements and failing to accurately identify the facility type can lead to improper testing protocol.
Leaving the contact information incomplete: Contact information for both the facility and the owner is crucial for any follow-up required. Sometimes, people either leave this section partially filled or provide outdated information, making it difficult for the radon program to get in touch if necessary.
Incorrectly calculating the number of measurements: The form requires respondents to state the number of measurements required and conducted within the testing period. Misinterpreting how many measurements are needed for the size and type of the building can lead to non-compliance with testing protocols.
Not checking all applicable boxes for the foundation/floor system or HVAC system: The building information section includes checkboxes for the details of the building’s foundation/floor system and HVAC system. Often, individuals will check only one box when in fact multiple options may apply, leading to incomplete information regarding the building's specifications.
Mistakes in the results section: This section is critical as it records the actual radon levels found during testing. Common mistakes here include entering incorrect measurement dates, failing to specify the unit of measurement, or inaccurately recording the radon level detected.
Failing to sign and date the form: Whether measurements are performed by a radon measurement business or by staff employed by the facility, the form requires a signature and date in sections 4 or 5 respectively. Overlooking this step can result in the form being considered incomplete.
By being aware of these common pitfalls and taking the time to review the form thoroughly before submission, individuals can ensure a smoother process in achieving compliance with Florida's radon testing requirements for nonresidential buildings.
Documents used along the form
Filling out the Florida DH 1777 form, which pertains to radon measurement in nonresidential buildings, is just one step in ensuring the safety and compliance of the facility with environmental and health regulations. Alongside this mandatory measure, several other documents and forms are often utilized to paint a complete picture of a facility’s adherence to standards, each serving a distinctive purpose in the broader context of environmental health management.
- Building Permit: Documents approval to begin construction or renovation, showing compliance with building codes.
- Radon Mitigation System Installation Records: Details on the installation of systems designed to reduce radon levels in the building, including the design and operational details.
- Occupancy Permit: Issued after construction, certifying that the building is safe for occupancy and complies with local codes and regulations.
- Environmental Impact Assessment (EIA): Analyzes the anticipated effects of the project on the local environment, including air quality considerations such as radon.
- Health and Safety Compliance Documents: Prove a facility’s adherence to various health and safety codes, potentially including measures taken to address radon exposure.
- Facility Maintenance Records: Logs of maintenance work conducted on the facility that could affect radon levels, such as HVAC system repairs or modifications.
- Radon Testing Kit Instructions: Manufacturer’s guide on how to correctly use radon testing kits, crucial for ensuring accurate measurement results.
- Quality Assurance/Quality Control (QA/QC) Plan: A document outlining procedures to ensure the reliability and accuracy of the radon measurement process.
- State or Local Radon Disclosure Forms: Required in some jurisdictions, these forms disclose radon measurement results to current or potential occupants.
- Employee Training Records: Prove that staff have been trained on radon awareness and safety, relevant to facilities managing their own measurements.
Collectively, these documents support a comprehensive approach to managing radon risks and maintaining regulatory compliance. They are essential both for the safety of people using the facility and for protecting the environment. Proper documentation ensures that all measures taken are appropriate, effective, and in line with both state and federal guidelines.
Similar forms
The Florida DH 1777 form is similar to other documentation used for reporting environmental health and safety concerns, specifically in the context of radon measurement in nonresidential environments. Two notable documents share commonalities with the Florida DH 1777 form: the EPA's (Environmental Protection Agency) Radon Measurement in Schools (second edition) and the ANSI/AARST MAH-2019 protocol for conducting radon and radon decay product measurements in multifamily buildings. Each of these documents, like the Florida DH 1777, guides the structured reporting of radon levels to ensure the safety and health of building occupants.
The EPA’s Radon Measurement in Schools (second edition) outlines step-by-step procedures for conducting and reporting radon measurements in school buildings. Similarly to the DH 1777 form, the EPA’s guide requires information on the facility's location, the specific areas tested, the type of radon detection devices used, and the results of those tests. However, the DH 1777 form is explicitly tailored for a broader range of nonresidential buildings, including schools. This means while both documents serve to protect public health by ensuring safe levels of radon, the DH 1777 form is adaptable for use beyond educational settings, encompassing facilities such as nursing homes, day care centers, and correctional facilities.
The ANSI/AARST MAH-2019, on the other hand, provides a comprehensive protocol for radon measurement in multifamily buildings, aiming to assess and manage radon risk in high-density housing. This document shares several procedural similarities with the DH 1777 form, including the requirement for detailed reporting of the facility and measurement locations, device types, testing duration, and specific outcomes of radon levels detected. While the DH 1777 encompasses a variety of facility types, the ANSI/AARST MAH-2019 strictly focuses on residential multifamily buildings. The DH 1777 form's broader applicability makes it a versatile tool for ensuring the safety of occupants across a wide array of nonresidential settings.
Dos and Don'ts
When you are tasked with filling out the Florida DH 1777 form, which is required for reporting radon measurements in non-residential buildings, there are crucial steps to follow and common pitfalls to avoid. Ensuring that this documentation is completed accurately and thoroughly is essential for complying with state regulations and for the safety of the facility's occupants. Here are four dos and don'ts to guide you through the process:
Do:
Read the instructions carefully before attempting to fill out the form. Each section has specific requirements that must be adhered to, and understanding these in advance can save time and prevent errors.
Provide complete and accurate information for both the facility and owner details in Section 1. This includes the facility name, physical location, contact person, owner’s name, and respective addresses and phone numbers. Incomplete or inaccurate information can lead to delays or complications in the handling of your report.
Ensure that all measurements and results reported in Section 3 are entered correctly, including the measurement type, dates, and results. Accurate reporting of this data is critical for the assessment of radon levels and the health and safety of the building's occupants.
Include the certification numbers where applicable. If the measurements were performed by a radon measurement business, the business and specialist’s certification numbers must be included in Section 4. This verifies that the measurements were conducted by qualified professionals.
Don't:
Leave any sections incomplete. This form acts as an official record and must be fully completed to comply with Chapter 64E-5, Florida Administrative Code, and Chapter 404, Florida Statutes. Even if a section seems not to directly apply, review it to be sure no part of it requires your input.
Guess on details or measurements. If you are unsure about any information, take the time to verify it. Providing guesses or inaccurate data can lead to non-compliance or a false assessment of the facility's radon levels.
Use abbreviations or jargon that are not universally recognized. While filling out the form, keep in mind that the information should be clear and accessible to everyone, including those who may not have a technical background in radon measurement or environmental health.
Forget to sign and date the form where required. A signature is required in Section 5 if the measurements are performed by staff employed by the facility, to certify that the radon measurements reported have been performed in accordance with relevant regulations. Unsigned forms will not be processed.
By following these guidelines, you can ensure that the Florida DH 1777 form is filled out correctly and thoroughly, meeting all regulatory requirements and contributing to the safety and well-being of the facility's occupants. If you have any questions or require assistance, do not hesitate to contact the Florida Department of Health’s Radon Program for support.
Misconceptions
One common misconception is that the Florida DH 1777 form is only required for residential properties. In fact, this form specifically targets nonresidential buildings other than single or multi-family dwellings, including facilities such as day care centers, schools, and hospitals, to report mandatory radon measurements.
Another misunderstanding is that only one measurement is required for the entire facility. However, the form outlines the necessity for individual measurements in each applicable building or section, specifying that measurements may be required both as initial testing and as part of a five-year retest or follow-up.
Many believe that the Florida DH 1777 form can be filled out and submitted by an owner or facility manager alone. While facility staff can perform the measurements, if the measurements are conducted by a radon measurement business, the details of the business and the specialist, including their certification numbers and the specialist’s signature, must also be included on the form.
It's often thought that once the form is completed and submitted, the obligation is fulfilled. However, this overlooks the requirement for the measurements to be carried out according to regulations set forth in Chapter 64E-5, Florida Administrative Code, and Chapter 404, Florida Statutes. Furthermore, the form must be sent to the specific address of the Department of Health's Radon Program or emailed to the designated address, ensuring proper processing and compliance.
Key takeaways
When dealing with the Florida DH 1777 form, which is required for reporting radon measurements in nonresidential buildings, understanding the correct way to fill out and submit the form ensures compliance with state regulations. Here are five key takeaways to assist in this process:
- Accurate Facility and Owner Information is Crucial: Section 1 of the form requests detailed information about the facility and its owner. This includes the facility name, physical location, contact person, type of facility, and owner’s information. It's important that this information is filled out accurately to ensure that the report is matched to the correct facility.
- Detailed Building Information is Required: Providing a comprehensive overview of the building's characteristics is necessary in Section 2. This includes the building name or ID, address, number of stories, foundation type, HVAC system details, and the building's age. Accurate reporting here helps in assessing the radon exposure risk correctly.
- Measurement Details Must Be Precisely Reported: Section 3 demands specific details about the radon measurements, including the type of measurement, dates, the person or entity performing the measurement, and the results. Using the correct units and including the certificate number if applicable is essential for the validity of the report.
- Identification of the Measurement Executor: The form differentiable between measurements performed by a radon measurement business (Section 4) and those conducted by staff employed by the facility (Section 5). Identifying who conducted the measurement is crucial, as it ties into the compliance and verification process outlined by Florida's radon legislation.
- Submission Process: Upon completing the form, it can be submitted either by mail to the Department of Health’s Bureau of Environmental Health / Radon Program or by email. The form provides specific addresses and email for submission, and also lists a contact number for assistance in filling out the form, ensuring that help is available for those who need it.
Understanding these key aspects of the Florida DH 1777 form not only aids in adhering to the state's health and safety regulations but also in protecting the wellbeing of individuals in various nonresidential buildings by ensuring accurate and responsible radon reporting.
Popular PDF Documents
Florida Proof Loss - A loss reporting document in Florida for insurance policyholders, mandating a comprehensive and truthful declaration of damages.
Florida Ucc1 - The Florida UCC1 form facilitates the introduction of new courses into the Statewide Course Numbering System, streamlining education standards.