Fill Out a Valid Florida Hospital Template
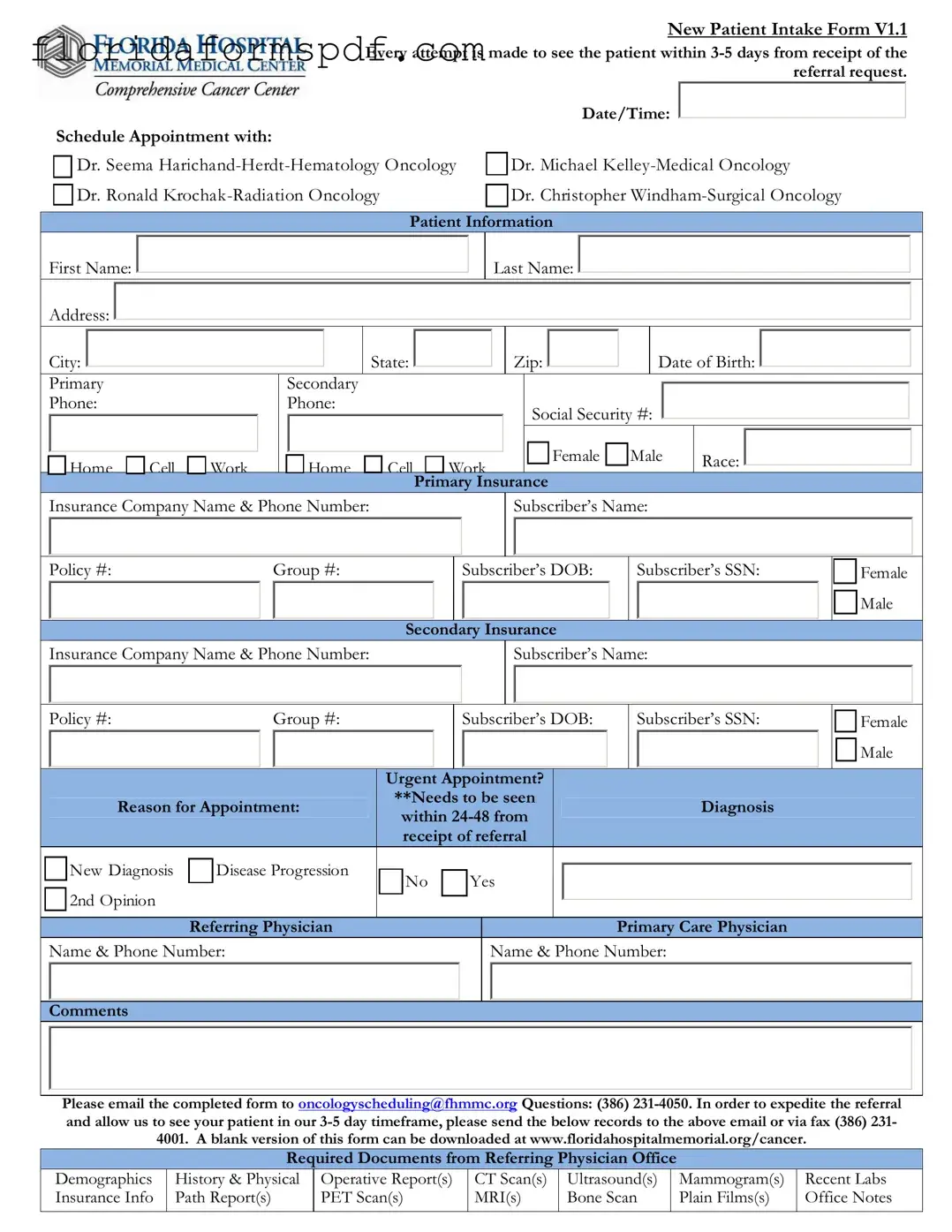
When it comes to navigating the healthcare system, especially for new patients at oncology centers, having a straightforward and efficient process is crucial. The Florida Hospital’s New Patient Intake Form V1.1 embodies this necessity by streamlining the referral process, aiming to schedule appointments within 3-5 days of receiving a referral request. This form is comprehensive, requiring detailed patient information including name, contact details, social security number, gender, race, and insurance information. It also delves into the specifics of the appointment—whether it is urgent, the reason behind it, and includes sections for both primary and secondary insurance details. Furthermore, it outlines the necessary documents needed from the referring physician's office such as demographic information, medical history, and various reports and scans that paint a complete picture of the patient’s health status. To ensure smooth communication and scheduling, it provides instructions for emailing the completed form and even includes a section dedicated to the cancer center scheduler to enter appointment details and patient information into their system. This form not only serves as a pivotal tool for the hospital’s administrative and medical staff but also signifies the hospital's commitment to providing timely and specialized care for patients navigating through a challenging period in their lives.
Document Preview Example
New Patient Intake Form V1.1 Every attempt is made to see the patient within
Schedule Appointment with: |
|
Date/Time: |
|
|
|
|||
|
|
|
||||||
|
|
|
|
|
||||
|
|
Dr. Seema |
|
Dr. Michael |
||||
|
|
|
||||||
|
||||||||
|
||||||||
|
|
Dr. Ronald |
|
|
Dr. Christopher |
|||
|
|
|
|
|||||
|
|
|
|
|||||
Patient Information
First Name: 

Address: 
Last Name: 


|
City: |
|
|
|
|
State: |
|
|
|
|
Zip: |
|
|
|
|
|
|
Date of Birth: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Primary |
|
Secondary |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Phone: |
|
Phone: |
|
|
|
|
Social Security #: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Home |
Cell |
Work |
Home |
Cell |
Work |
Female |
Male |
Race: |
|
|
|
|
|
Primary Insurance |
|
|
|
|
|
Insurance Company Name & Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber’s Name: |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy #: |
|
|
|
Group #: |
|
|
|
|
|
|
|
Subscriber’s DOB: |
|
|
Subscriber’s SSN: |
|
|
Female |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Secondary Insurance |
|
|
|
|
|
|
|
|||||||||||||||
|
|
Insurance Company Name & Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber’s Name: |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Policy #: |
|
|
|
Group #: |
|
|
|
|
|
|
|
Subscriber’s DOB: |
|
|
Subscriber’s SSN: |
|
|
Female |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Urgent |
|
|
|
|
|
Appointment? |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
**Needs to be seen |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
Reason for Appointment: |
|
|
|
|
Diagnosis |
|
|
|
|
||||||||||||||||||||
|
|
|
|
within |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
receipt of referral |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
New Diagnosis |
|
Disease Progression |
|
No |
|
|
|
|
Yes |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
2nd Opinion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referring Physician |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary Care Physician |
|
|
|
|
||||||
|
|
Name & Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
Name & Phone Number: |
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please email the completed form to oncologyscheduling@fhmmc.org Questions: (386)
|
|
|
|
|
|
|
|
|
|
|
|
Required Documents from Referring Physician Office |
|
|
|
||||
|
Demographics |
History & Physical |
Operative Report(s) |
CT Scan(s) |
Ultrasound(s) |
|
Mammogram(s) |
Recent Labs |
|
|
Insurance Info |
Path Report(s) |
PET Scan(s) |
MRI(s) |
Bone Scan |
|
Plain Films(s) |
Office Notes |
|
Patient Label
THIS SECTION TO BE COMPLETED BY THE CANCER CENTER SCHEDULER
PATIENT INFORMATION
|
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
APPOINTMENT DATE/TIME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CARE NAVIGATORS NOTIFIED |
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breast Care Navigator |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Appt Date: |
|
|
|
|
|
|
|
|
|
|
|
Appt Time: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lung Care Navigator |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
PATIENT AND APPOINTMENT ENTERED INTO SYSTEM |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
Radiation Oncology (Dr. Krochak) |
|
|
|
|
|
|
Dr. Harichand, Dr. Kelley, Dr. Windham |
|
|
|||||||||||||||||||||||||
|
MR # |
|
|
|
|
|
|
FIN# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Cerner Scheduling |
|
|
IMPAC |
|
|
|
ARIA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
PATIENT NOTIFIED |
|
|
|
|
|
|
|
|
NEW PATIENT PACKET GIVEN TO PT |
|
|
||||||||||||||||||||||||||||
|
Date/Time Patient Notified: |
|
|
|
CCC General Pt Packet |
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailed |
Date/Time: |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
Spoke directly to patient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Spoke with patients family |
|
|
|
|
|
|
|
|
|
|
Emailed |
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
RECORDS RECEIVED FROM REFERRING PHYSICIAN |
|
|
|
|
|
|||||||||||||||||||||||||||
|
Date: |
|
|
|
|
|
|
|
|
|
|
Pathology Report |
|
|
|
Operative Report |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Applicable Consultation Reports |
|
|
Bone Scan |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
History & Physical |
Most Recent Blood Work (Labs) |
|
CT Scan |
|
|
|||||||||||||||||||
|
Time: |
|
|
Initials: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PET Scan |
|
|
|
|
|
|
MRI |
|
|
Mammogram |
|
Ultrasound |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHART CREATED |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Radiation Oncology (Dr. Krochak) |
|
|
|
|
|
|
Dr. Harichand, Dr. Kelley, Dr. Windham |
|
|
|||||||||||||||||||||||||||||
|
Chart Label printed (Name & MRN) |
|
|
|
|
|
|
|
|
|
|
Chart Label printed (Name & DOB) |
|
|
|
|
|
|||||||||||||||||||||||
|
Facesheet & Labels printed from Cerner |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
Records in chart |
|
|
|
|
|
||||||||||||||||||||||||||||
|
Records in chart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
CHART FORWARDED TO NURSING |
|
|
|
|
|
|
|
|
|
|
|
|
NURSING RECEIVED |
|
|
||||||||||||||||||||||||
|
Date/Time: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initials: |
|
|
|
|
|
Date/Time: |
|
|
|
|
|
Initials: |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Notes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Document Overview
| Fact | Detail |
|---|---|
| Form Version | New Patient Intake Form V1.1 |
| Scheduling Timeframe | 3-5 days from receipt of referral request |
| Specialists Listed | Dr. Seema Harichancer-Herdt, Dr. Michael Kelley, Dr. Ronald Krochak, Dr. Christopher Windham |
| Patient Information Required | First Name, Last Name, Address, Phone Numbers, Social Security Number, Date of Birth, Gender, Race, Insurance Details |
| Insurance Information Required | Primary and Secondary Insurance Details including Company Name, Subscriber's Name, Policy and Group Numbers, Subscriber's DOB and SSN |
| Urgent Appointment Criteria | Needs to be seen within 24-48 hours for reasons like New Diagnosis, Disease Progression, or for a 2nd Opinion |
| Referral Documentation Required | Demographics, History & Physical, Operative Report(s), CT Scan(s), Ultrasound(s), Mammogram(s), Recent Labs, Insurance Info, Path Report(s), PET Scan(s), MRI(s), Bone Scan, Plain Films(s), Office Notes |
| Governing Law(s) | Health Insurance Portability and Accountability Act (HIPAA), Florida Patient's Bill of Rights and Responsibilities |
Instructions on How to Fill Out Florida Hospital
Completing the Florida Hospital New Patient Intake Form is an essential step in ensuring that you or your loved one receives timely and efficient care. This process helps the medical team understand the patient's health background, insurance details, and the reason for the appointment, facilitating a smoother visit and more tailored care. Accurately filling out this form is critical for setting up an appointment with the appropriate specialist, whether it be in Hematology Oncology, Medical Oncology, Radiation Oncology, or Surgical Oncology. Here's how to fill out the form:
- Start by selecting the specialist you need an appointment with: Dr. Seema Harichand-Herdt for Hematology Oncology, Dr. Michael Kelley for Medical Oncology, Dr. Ronald Krochak for Radiation Oncology, or Dr. Christopher Windham for Surgical Oncology. Note the preferred date and time.
- Under the Patient Information section, enter the patient's first name, last name, address (including city, state, and ZIP code), date of birth, and social security number.
- Provide contact information, including both a primary and secondary phone number. Indicate whether each number is a home, cell, or work number.
- Specify the patient's gender and race.
- For both Primary and Secondary Insurance sections, input the insurance company name, phone number, subscriber's name, policy number, group number, subscriber's date of birth, and social security number. Mark the gender of the subscriber as well.
- Check the box if the appointment is urgent, necessitating a visit within 24-48 hours, and specify the reason for the appointment (New Diagnosis, Disease Progression, 2nd Opinion).
- Fill in the referring physician's and primary care physician's names and phone numbers, and add any relevant comments concerning the patient's condition or specific needs.
- For the cancer center scheduler to complete, note the date and time of the scheduled appointment along with information about the Care Navigators notified.
- Ensure that all required documents listed in the form are gathered from the referring physician's office and sent to the provided email or fax number.
- Check the box corresponding to the communication method used to notify the patient about the new patient packet and the appointment details.
- Lastly, record the date and time when the patient's records were received from the referring physician, including any consultations, reports, scans, labs, and the chart's status in the medical system.
Once the form is thoroughly completed, it should be emailed to the specified address. This step is crucial for ensuring that the healthcare team has all the necessary information to provide the best possible care tailored to the patient's specific conditions and needs. Timely submission of the form and any accompanying documents accelerates the intake process, helping the patient to receive the necessary medical attention without unnecessary delays.
Listed Questions and Answers
What is the purpose of the New Patient Intake Form V1.1 for Florida Hospital?
The New Patient Intake Form V1.1 is a critical document designed to gather essential information about a new patient at Florida Hospital. The primary purpose of this form is to streamline the process of referral, ensure that the patient's appointment is scheduled with the right specialist, and see that all necessary medical records are prepared and presented at the time of the appointment. The form captures basic patient information, insurance details, the urgency of the appointment, the reason for the appointment, and relevant medical history to facilitate a quick and efficient intake process.
How quickly does Florida Hospital aim to schedule an appointment after receiving a referral?
Florida Hospital endeavors to schedule appointments within 3-5 days from the receipt of the referral request. This quick scheduling is part of the hospital's commitment to providing timely care, especially in urgent cases or for patients needing prompt evaluation and treatment. The form explicitly asks whether an appointment is urgent, indicating whether a patient needs to be seen within 24-48 hours from receipt of referral, ensuring that urgent cases are given priority.
What types of specialists can appointments be made with using this form?
Appointments can be made with specialists in Hematology Oncology, Medical Oncology, Radiation Oncology, and Surgical Oncology. These specialist areas cover a wide range of cancers and related diseases, allowing referrals to be tailored to the patient's specific diagnosis and treatment needs. Each specialist listed, including Dr. Seema Harichand-Herdt, Dr. Michael Kelley, Dr. Ronald Krochak, and Dr. Christopher Windham, brings a wealth of experience and expertise to the care team.
What information is needed from the referring physician's office?
To expedite the referral and ensure that the Florida Hospital care team is prepared for the new patient's appointment, the form requests several documents from the referring physician's office. These include the patient's demographic details, their medical history, any operative reports, imaging results such as CT scans, ultrasounds, mammograms, recent laboratory tests, insurance information, pathology reports, PET scans, MRIs, bone scans, plain films, and office notes. Collecting this information in advance helps the care team to make informed decisions and recommendations during the initial appointment.
How is the patient informed about their appointment details?
Once the appointment is scheduled, the patient is notified about the date and time. The form provides space for detailing how the patient was informed (direct conversation, through a family member, or by email), ensuring clear communication. Additionally, the patient is given a new patient packet, which can be mailed or emailed, containing information to prepare for the visit, such as what to expect, directions to the facility, and any pre-appointment instructions or paperwork that needs to be completed. This proactive communication helps to ease patient anxiety and ensures they come prepared for their visit.
Common mistakes
- Not providing complete contact information: When filling out the form, a common mistake is leaving sections like primary and secondary phone numbers blank or incomplete. This can hinder communication efforts, delaying the scheduling process or follow-up care.
- Incorrectly filling out insurance details: Patients often enter incomplete or incorrect information regarding their primary and secondary insurance. It's crucial to input accurate details such as the insurance company name, policy number, group number, and the subscriber's information to ensure smooth processing and coverage validation.
- Overlooking the urgency of the appointment: Failing to properly indicate whether the appointment is urgent can lead to significant delays in receiving necessary care. If the appointment is marked as non-urgent when it actually is, it may not get scheduled within the critical 24-48 hour window needed for urgent cases.
- Not including the required documents from the referring physician: Another critical oversight is not attaching or sending the required documents such as the patient's demographics, history & physical, recent labs, and insurance information. These documents are vital for the cancer center to fully understand the patient's situation and to prepare for their visit adequately.
Documents used along the form
When a patient is referred to a hospital in Florida, a comprehensive approach is taken to ensure that all necessary information is gathered to facilitate their care. Alongside the Florida Hospital form, several other forms and documents are commonly used to complement the patient's medical and administrative records. These documents are essential for a seamless healthcare experience, offering a complete view of the patient’s health history, insurance details, and specific medical needs. Below is a list of documents often used in conjunction with the Florida Hospital form.
- Advance Directive Forms: These documents, including living wills and health care surrogate designations, specify a patient's preferences regarding medical treatments and interventions in situations where they cannot make decisions for themselves.
- Consent to Treat Forms: This essential document is signed by the patient or a legal guardian to give the medical team permission to administer treatment, including surgeries, procedures, and other care plans.
- Medical Records Release Form: Used to authorize the release and sharing of a patient’s medical records between healthcare providers. It ensures that all pertinent medical history is available to the treating physicians and specialists.
- Medication List: A comprehensive document detailing all medications a patient is currently taking, including dosage and frequency. This list aids in preventing prescription errors and drug interactions.
- Financial Agreement Forms: These documents outline the financial responsibilities of the patient, including details on insurance coverage, payment plans, and policies for uninsured patients. It ensures transparency regarding the costs associated with healthcare services.
- Privacy Notice Acknowledgement Form: It acknowledges that the patient has received the Notice of Privacy Practices, informing them about how their medical information may be used and disclosed and how they can access this information.
- Insurance Cards and ID: Copies of the patient’s insurance card(s) and a valid form of identification, like a driver’s license, are often required to verify insurance coverage and for billing purposes.
Collecting and managing these documents is crucial for the coordinated effort needed to deliver effective patient care. They not only support the logistical and administrative aspects of healthcare provision but also ensure that the patient's treatment plan is well-informed and personalized to their specific needs. By maintaining a comprehensive and up-to-date patient file, healthcare providers can improve the quality of care, enhance patient safety, and streamline communication among the care team.
Similar forms
The Florida Hospital form is similar to standard medical intake forms used in various healthcare settings. Like those forms, it gathers essential information about the patient, including personal identification details, contact information, insurance information, and medical history. Both sets of documents typically require the patient's name, address, date of birth, phone numbers, and insurance details. Furthermore, they inquire about the reason for the current visit, such as a new diagnosis or the progression of an existing condition. The aim is to streamline the patient's entry into the healthcare system, ensuring that all relevant information is captured efficiently to facilitate care planning and coordination.
Another document that the Florida Hospital form resembles is the referral request form that healthcare providers use when sending a patient to a specialist. These forms contain sections for the referring physician's information, reasons for the referral, and urgent appointment indicators, similar to the Florida Hospital's form directives on seeing the patient within a specific timeframe and the need for an urgent appointment based on a new diagnosis or disease progression. Both documents serve the crucial function of ensuring a smooth transition of care from the referring physician to the specialist, including the sharing of necessary medical documents such as history and physical, lab results, and imaging studies to support an informed consultation.
Moreover, the form shares similarities with specialized oncology intake forms, particularly in its detailed request for information regarding the patient's cancer diagnosis, treatment history, and specific oncology-related documents. These include operative reports, CT scans, and more, which are critical for oncology care. Such forms also stress the importance of including insurance information due to the often high costs associated with cancer treatment. The aim here is to gather comprehensive information pertinent to the patient's cancer diagnosis and treatment plan, ensuring that the oncology team has all necessary details to provide specialized and timely care. This focus on detailed medical history, especially related to cancer, underscores the role of these forms in supporting the complex clinical decision-making process inherent in oncology.
Dos and Don'ts
When filling out the Florida Hospital New Patient Intake Form, there are specific steps you should follow to ensure the process goes smoothly and your form is processed efficiently. Here are five quintessential dos and don’ts to consider:
Things You Should Do:
Double-check that all personal information (such as name, address, date of birth, and phone numbers) is accurate and matches your identification documents.
Ensure all insurance information, including the company name, policy number, and the subscriber's information, is filled out completely and correctly.
Clearly indicate the urgency of the appointment if it’s an urgent appointment, by marking "Yes" for the question pertaining to needing an appointment within 24-48 hours from receipt of the referral.
Include the reason for the appointment, such as a new diagnosis or a second opinion, to provide the scheduling team with clear context.
Email the completed form to the provided oncology scheduling email address, and confirm receipt with the hospital by calling the provided phone number if necessary.
Things You Shouldn’t Do:
Leave any sections blank, especially those related to patient information or insurance details, as incomplete forms may delay processing.
Forget to attach or send any required documents listed under the 'Required Documents from Referring Physician Office' section.
Use nicknames or incomplete names – always provide full legal names as they appear on your insurance and identification documents.
Ignore the email confirmation step after initially submitting your form, as this is critical to ensure your form has been successfully received.
Provide outdated contact information or phone numbers that might make it difficult for the hospital to reach you for confirmation or additional information.
Following these guidelines will contribute to a smoother intake process, enabling the hospital staff to schedule your appointment more efficiently and ensuring that all necessary information for your care is ready and available.
Misconceptions
When discussing the New Patient Intake Form utilized by Florida hospitals, several misconceptions often emerge. Recognizing and understanding these misconceptions is vital for ensuring that both patients and healthcare providers navigate the process efficiently and with clarity.
- Misconception 1: All New Patient Forms Are Essentially the Same
One common misconception is the belief that new patient forms for all hospitals in Florida, or even within the same healthcare system, are identical. However, the New Patient Intake Form, as shown with the version 1.1, can vary significantly not just by hospital but also by department within a hospital. These forms are tailored to gather specific information necessary for the unique workflow and information requirements of each specialty, such as Hematology Oncology, Medical Oncology, and Surgical Oncology among others specified in the form.
- Misconception 2: Submission of the Form Guarantees an Appointment within 3-5 Days
While the form states that "every attempt is made to see the patient within 3-5 days from receipt of the referral request", many assume this timeframe is guaranteed. However, this is an ideal goal and can be impacted by the urgency of the appointment, the capacity of the facility, or the availability of the requested physician. Although the hospital aims to accommodate this timeframe, it is not always possible, especially in cases requiring urgent attention which are prioritized.
- Misconception 3: Email is the Only Method for Form Submission
Another misconception is that the completed form can only be submitted via email. While email is a primary method for form submission, as indicated by the provision of the oncologyscheduling@fhmmc.org email address, the form and accompanying documents can also be sent through fax. This flexibility accommodates different preferences and ensures the form can be submitted in a manner most convenient or accessible to the referring physician or office.
- Misconception 4: Patient Responsibility Ends After Form Submission
Lastly, there's a misconception that once the form has been submitted, the patient’s role is entirely passive in the scheduling process. The form clearly mentions a section for patient notification and the provision of a new patient packet, indicating an active, ongoing communication process between the patient (or the patient's family) and the hospital. It underscores the importance of continued engagement by the patient or their advocates to confirm appointments, understand next steps, and prepare for the visit.
Understanding these common misconceptions can greatly improve the experiences of both patients and healthcare providers by setting realistic expectations and encouraging proactive communication throughout the new patient intake process.
Key takeaways
Filling out and using the Florida Hospital form for new patient intake, especially within the oncology departments, involves a defined procedure to ensure timely and organized medical care. Understanding the steps and information required can help streamline the process for both patients and healthcare providers. Here are key takeaways:
- The form prioritizes urgent appointments, indicating that patients with a new diagnosis or who are experiencing disease progression, and require an evaluation within 24-48 hours from the referral, should be clearly marked as needing urgent attention.
- Comprehensive patient information is necessary for a holistic approach to patient care. This includes basic personal information, detailed contact information, social security number, and both primary and secondary insurance details to facilitate billing and verification processes.
- Effective communication between referring physicians and the oncology department is facilitated through the provision of a specific email address and fax number for submitting the completed form and accompanying documents. These documents include demographics, medical history, operative reports, recent labs, imaging studies, and insurance information to aid in the pre-appointment preparation.
- The process of booking an appointment and preparing the patient's chart for the visit is systematic. The form details the steps to be taken by the cancer center scheduler upon receipt of the referral, from entering patient information into the system and notifying care navigators to preparing the new patient packet and notifying the patient about the appointment details.
Overall, filling out the Florida Hospital form thoroughly and accurately is crucial for ensuring that patients receive timely and coordinated care tailored to their specific oncological needs. This structured approach helps streamline the intake process and aids healthcare providers in delivering high-quality care.
Popular PDF Documents
How to Become a Cna in Florida - Submission details for additional documents and updates required post-application for CNA licensure in Florida.
Dh 681 Form - Ensures legal compliance with Sections 1003.22, 402.305, 402.313 of the Florida Statutes and associated administrative codes.